Close the Gap: Bladder Cancer
A symptom may be the first red flag.
Bladder cancers often hide in plain sight.
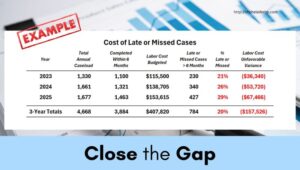
Bladder cancer cases surface from the inpatient and outpatient settings, each telling a story that pathology alone cannot capture. When casefinding workflows depend only on positive pathology, clinically diagnosed or recurrent cases are easily overlooked. Each omission distorts the cancer registry’s accuracy and the facility’s performance.
Patients may present with negative pathology or pathology performed elsewhere. Others are seen with partial treatment delivered elsewhere, surveillance, or recurrence documented outside of the primary EMR. A patient returning for intravesical therapy, transurethral resection, or follow-up cystoscopy after a prior diagnosis may not have a new tissue confirmation but still meet the criteria for a reportable case.
Use of all relevant ICD-10 codes from the medical disease indices (MDI) is critical and includes:
—New or primary diagnosis: C67.x
—Symptoms at time of admission or suggestive of recurrence: R31.x, Z85.51, Z48.3
—Procedural ICD-10-PCS codes: 0TJB8ZZ, 0TB88ZX, 0TJB8ZZ, 0TBB8ZX, 0TBB8ZZ, 0T9B8ZX, 3E0M3GC.
—Surveillance and follow-up codes: Z85.51, Z08, Z48.3, Z09, Z51.11, Z51.0, Z48.816,
SEER data confirms that symptom-based encounters, especially hematuria, are a frequent entry point for bladder cancer detection in older adults (Fankhauser et al., 2023). NAACCR similarly emphasizes that completeness depends on capturing clinically diagnosed and recurrent cases from non-pathology sources such as cystoscopy, consults, and discharge summaries (NAACCR, 2024).
AI-driven casefinding unites data streams, pathology, imaging, and medical indices, into a single, complete and efficient workflow. Automation reduces human error, improves timeliness, and ensures every case is visually reviewed by the cancer registrar.
Actionable Tip: Ensure the cancer registry casefinding practices are surfacing all reportable bladder cases by:
—Review MDI filters ensuring all ICD-10 disease codes and PCS procedural codes are up-to-date.
—Audit unfiltered MDI’s. Compare encounters with ICD-10 and procedural codes to the registry accession registry.
—Prepare a final report with results and an action plan. Share with administrator and Cancer Committee.
Close code gaps and strengthen the cancer registry’s reach by connecting ICD-10 codes and EMR data to patient care to ensure every bladder cancer case is collected and reported.
First published on LinkedIn.
\ Get the latest news /